
Posted by Behavioral Health Billing Solutions, LLC.

Let’s talk about Behavioral Health agency Billing NPI’s.
Several years ago, Ohio Medicaid went to Behavioral Health agencies needing to create a separate Billing NPI to separate out Mental Health services from Alcohol and Drug or as now referred to Substance Abuse disorders. Prior to that time, most agencies providing both types of services billed under what I call their “forever NPI”.
For most, that was the Billing NPI they also used to bill Insurance and panel with Medicare. When Medicaid required the split between the two lines, it did not apply to how they billed Insurance and Medicare.
Agencies adjusted to this change rather easily, even though it was a significant change to how they billed Medicaid.
As of July 1st, 2018, Ohio Behavioral Health agencies had to start billing the Managed Care agencies directly if the client did not have fee for service Medicaid, which is the bulk of the client base. ODM required the MCO’s to also change their process to bill SUD and MH services under the appropriate Billing NPI. The tricky part is several of the MCO’s could not adjust their adjudication process to look for the Billing NPI verses the type of service and deny when services were billing incorrectly for the type of service being provided.
What has happened is multi-layered:
First, most agencies were used to billing Ohio Medicaid under two different NPI’s, however, it appears that some didn’t understand that MCO’s were under the same rules are ODM and they are billing under “their forever NPI”. In some cases, they are receiving payment, even though it is incorrect.
However, MCO’s like Molina, were able to correct their adjudication to accurately reflect the change required by ODM. They simply aren’t paying for services billed under one NPI when it is obviously a different type of service and this is an appropriate and correct denial being applied to those services.
Let’s talk about the second issue I am seeing due to this difference.
Many agencies seem to have experienced some additional confusion regarding the addition of this second NPI. The purpose of the addition was to differentiate services for Medicaid and the MCO’s. It does not apply to Insurance or Medicare.
We have been working with several agencies who applied the dual Billing NPI thought process to Insurance and Medicare. The result is absolute confusion with those payers and total claim denials from Medicare, which I’ve seen, and most likely the same issue with Insurance but I am seeing less problems with this area.
Depending on your interpretation of these changes, it’s possible you are experiencing payment issues with some of the MCO’s and definitely an issue with Medicare and most likely, Insurance as well.
So nuts and bolts are; how do you identify if this is an issue for your agency?
-
Check with your billing and IT departments and see if they are aware that the MCO’s require you to bill SUD and MH services under the appropriate NPI for those services, in addition to the rendering NPI for all providers. If you aren’t set up this way, use the contact list below to reach out to the MCO’s to understand their policy related to this and then contact your EHR vendor to correct the issue efficiently.
-
The contact information is here to find out who to reach out to.
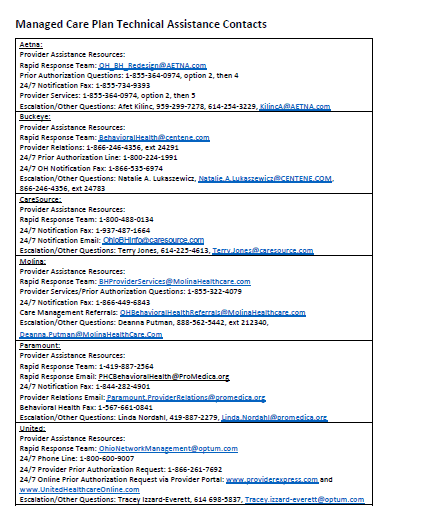{kind=link}
-
If you contract with Insurance, verify how you are contracted. What agency Billing NPI did you contract under? Have you seen denials for services stating incorrect or invalid practice like MA112 Missing/incomplete/invalid group practice information or maybe N95 incorrect provider?
-
If you bill Insurance, because now we have to, but aren’t contracted, this issue will be less easy to catch because most services deny anyway.
-
If you are contracted with Medicare, check and see whether or not you are receiving payments. IF you are receiving no payments and a denial code of MA112 on your 835 or EOB’s, it’s possible you contracted with them under both NPI’s. This causes a massive problem with Medicare that results in a lack of payment, at all, regardless of service type.
However, there is a somewhat easy correction. Keep in mind, nothing with Medicare is immediate and will probably involve you completing a new 46 page contracting document and possibly submitting a letter stating that you wish to remove the new NPI from your Medicare contract. In addition, you will need to contact them directly, have them specifically look at documented denials and verify how you are contracted. It’s not easy, however, it is doable. We had one agency who experienced this and was able to get the corrections up and functional and payments received within about a month, in conjunction with multiple, document submissions.
In addition to these issues, we have seen many instances of confusion regarding the differences between billing MCD January 2018 – June 2018 and post July 1st, 2018. The biggest difference is Jan – June 2018, only your independent providers should be billed with a rendering NPI.
Most systems, like Carelogic, have totally different EDI files that need to be used, in conjunction with some type of functionality to only include independent provider NPI’s during that time period.
As of July 1st, 2018, agencies are required to bill all services under the NPI of the rendering provider including independent, dependent and unlicensed. It was a massive change that included registering all providers with Medicaid under their credentials and roster those providers with each MCO.
Big changes are coming this month that will assist with how your providers are registered. It’s critical that all agencies pay attention to these positive changes and attend the training’s being offered so you know how to fully utilize these changes.
Please enroll in the webinar here.
The webinar will share important information related to the use of this file which will be available online at: https://bh.medicaid.ohio.gov/manuals beginning March 25th. By the way, the manual was recently updated on February 22nd so I recommend everyone goes out and reviews it thoroughly for changes that have occurred.
And keep in mind, as of January 1st, 2018, all CPT codes services must be billed to your client’s insurance first, regardless of whether you are contracted. Now there is a new issue with the use of CO96 to bill denied or no response insurance claims second to Medicaid and the MCO’s. We’ve been using CO96 in this manner for 5 years but apparently now, they are stating that this code is inappropriate unless an EOB has been received that states this particular denial reason or something to that effect. This is a substantial issue that has been brought up to ODM but as of right now, it remains unresolved. If you are currently using that code to bill next, I recommend you check your secondary claims are paying as expected for any that include a CAS code of CO96.
As always, BHBS is here to assist with any questions you might have. Please feel free to reach out if assistance is needed.